
Navy Medicine via Flickr
Lessons Learned from the COVID-19 Pandemic

Rebecca Emeny
Dartmouth Institute of Health Policy and Clinical Practice
Rebecca Emeny, PhD, MPH, is a Research Scientist and Teaching Faculty at The Dartmouth Institute of Health Policy and Clinical Practice. Rebecca received her undergraduate degree in Science, Technology and Society from Cornell University and her graduate degree in biomedical science from the University of New Mexico School of Medicine. She is a translational researcher with doctoral and post-doctoral training in microbiology/immunology and molecular epidemiology with expertise in neuroimmune mechanisms of chronic disease, resilience, and wellbeing in aging.
Dr. Emeny received her Master of Public Health at the Ludwig Maximilians University (LMU) in Munich, Germany and worked as the deputy director of the mental health working group of the Institute of Epidemiology of the Helmholtz Zentrum Muenchen from 2009-2015. Over her career, Rebecca has transitioned from experimental to observational studies in order to understand underlying mechanisms of chronic, non-communicable disease. Dr. Emeny is committed to applying this knowledge in patient and community centered research that enhances individual and population resiliency in order to improve public health and sustainable global health equity.
A U.S. Public Health Perspective
One month shy of two years into a global pandemic caused by the novel Severe Acute Respiratory Syndrome Associated Coronavirus 2 (SARS-CoV-2), with news of new variants and next waves, this AGI forum is a welcomed opportunity to take stock of where we are, where we’ve come from, and to reflect on lessons learned to move forward towards the noble goal of regional, national, and international health equity. This assessment is informed by the author’s experience as a scientist and a public health educator. As a molecular epidemiologist, I am interested in the cellular and molecular mechanisms that lead to pathologies that drive disease. Amidst all that I have learned during these pandemic times, I have benefited greatly from the perspectives of students I have had the privilege to teach. The past three years have brought about a three-fold increase in applications from students seeking a master’s degree in public health from our institution, which is a trend that has been observed across the nation.[1] These individuals are interested in understanding social risks and systemic injustice as drivers of health and disease as much as cancer, hypertension, and diabetes. They have witnessed the pandemic—many from the front lines of care—in their training as emergency medical technicians, nurses, and doctors. These experiences have motivated them to expand their knowledge base into foundations of public health, to inquire and learn about complex social, political, and economic “upstream” exposures that impact health outcomes. We teach these students skills that support the ten essential services of public health that revolve around three central activities; the assessment of health risks, the development of policy to inform and strengthen approaches to mitigate harm and improve health, and assurance provisions to ensure that efforts are sustainable in order to maintain “…a system in which all people can know and develop to their full potentials“.[2][3][4] It is with this perspective that my reflections of the COVID-19 pandemic experience focus on the following three factors; 1) the importance of rigorous, data-driven knowledge to inform evidence-based medical practice and public health initiatives, 2) the necessity of the measurement, risk communication, and management of social risk as much as biomedical risk, and 3) the value of a precision health framework, rather than a disease management framework, to guide the efforts needed to achieve the goals of public health.[5]
To exemplify and address the first factor of utilizing data wisely, the Johns Hopkins University Coronavirus Resource Center has from the onset, provided a robust real-time accounting of publicly reported data to describe and inform the public about the prevalence of SARS-CoV-2 identified infections and deaths related to the associated disease, COVID-19.[6] It was clear from the start, based on different regional and national approaches to public health management and messaging that testing and tracing along with avoiding close physical contact indoors and wearing face masks would reduce the likelihood of infectious spread of the virus. While both the United States[7] and South Korea[8] reported their first positive case at the end of January 2020, three months later in April, the COVID-19 Dashboard indicated that the case load in the United States was 40 times higher. And despite the availability of knowledge derived from digital infrastructures and health data analyses, the United States has now witnessed a loss of life that is among the highest in upper-middle and high-income countries (i.e. regions with reliable and complete mortality data), magnitudes 4-6 times greater than past influenza seasons.[9]
The COVID-19 pandemic has exposed tremendous variation in government responses as well as glaring disparities of health and access to health care in communities locally, regionally, nationally, and globally.
Regarding the second factor of risk communication throughout the pandemic, data quickly demonstrated that larger metropolitan regions were hardest hit initially, and carefully conducted epidemiologic studies provided evidence that asymptomatic individuals could transmit virus,[10][11] that viral transmission primarily occurred between close indoor contacts,[12] and that individuals with pre-existing diseases were at highest risk.[13][14] Nonetheless, widespread community testing was slow to become established and the concept of “social distancing” was ubiquitously promoted to “stop the spread“—a public health measure that has taken a severe toll on individuals’ mental health due to the stress imposed by social isolation in addition to the mental health burden typical of coronavirus pandemics.[15]
The COVID-19 pandemic has exposed tremendous variation in government responses as well as glaring disparities of health and access to health care in communities locally, regionally, nationally, and globally. My research, along with that of many others, has provided evidence that health disparities are driven by persistent toxicities of social and environmental stress exposures that accumulate across a lifespan and contribute to developmental immunotoxicity, chronic stress, inflammation, and intracellular pathologies that lead to ill-health and disease.[16] Research on the biologic consequences of psychosocial stress and social inequities is decades old,[17][18] as well as the awareness that one’s zip code has as much, if not a greater impact on one’s health than one’s genetic code.[19][20][21] This prompted the World Health Organization (WHO) to establish the Commission on Social Determinants of Health and in 2008 defined social determinants of health (SDOH) as “the conditions in which people are born, grow, work, live, and age.” The Commission recognized that the universal improvement of these conditions of daily living would be integral to achieving health equity.[22] The past two years have demonstrated that it is largely social determinants that have contributed to COVID-19 related mortalities. Indeed, at the peak of the pandemic in New York City neighborhoods, mortality rates were not evenly distributed; COVID-19-related mortality was higher in older populations and populations living with lower incomes and lower quality of health.[23]
Thus, reflecting on the third factor of a principled framework to guide and improve health care moving forward, it is interesting to consider a Precision Health approach. Precision health is a concept that links clinical practice, biomedical and epidemiologic research, and public health with the goal of “a unified approach to match a full range of promotion, prevention, diagnostic, and treatment interventions to fundamental and actionable determinants of health; to not just address symptoms, but to directly target genetic, biological, environmental, and social and behavioral determinants of health.”[24] After centuries of healthcare delivery focused solely on the treatment of a medical condition, the WHO now defines health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.”[25] This reframing of health has been necessary to incorporate a growing evidence base for the role of social and environmental context as key regulators of epigenetic, genetic, and molecular determinants of disease.[26] In some accounts, it has been suggested that clinical care impacts a mere 10 percent of one’s individual health, while factors such as genetics, personal behavior, and social and environmental issues account more or less equally to the rest.[27]
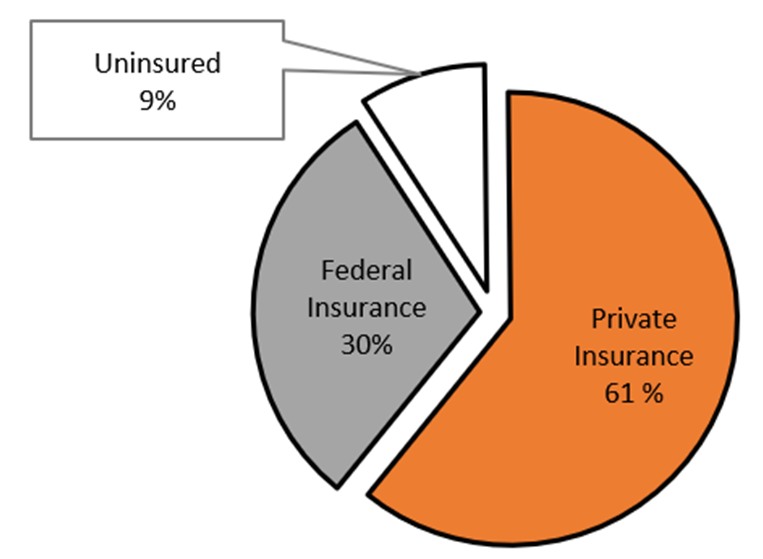
When considering the major differences between Germany and the United States, two main juxtaposing factors to consider are medical insurance coverage and digitization of health data. Germany has universal health care coverage and nearly no digitization, as pointed out by Arentz and Laufer, while America has (nearly) universal digitization of hospital-related health data and no universal medical insurance coverage. According to the 2020 census data, 8.6 percent of Americans are uninsured, and among the 91.4 percent of people in the United States with medical insurance; the majority (66.5 percent) received private insurance which is predominantly employment-based. Approximately a third of Americans received federally funded insurance—18.4 percent Medicare (for older individuals), 17.8 percent Medicaid insurance (for individuals with low income and/or disabilities) and 0.9 percent were covered by Veterans Affairs.[28] See Figure 1. Because older individuals and individuals living with low income were most susceptible to severe outcomes related to SARS-CoV-2 infection, the federal government has incurred a large portion of the health care costs of the pandemic.[29] The Healthcare Cost and Utilization Project used inpatient data from thirteen States to demonstrate that COVID-19-related hospitalizations were more likely to be billed to Medicare and less likely to be billed to private insurance (i.e., more than 10 percent lower) in May to September 2020 compared to all hospitalizations in April through September 2019.[30] Considering this distribution of medical insurance payment models, I will briefly describe the forces that led to the digitization of hospitals in the U.S. healthcare system and present efforts that have been launched locally and nationally to utilize patient data to improve health care services for both patients and providers.
Figure 1: Distribution of Health Insurance Coverage from 2020 United States Census Data (adapted from Keisler-Starkey et al. 2021)[31]
Digitization of hospitals in the United States
In the United States, federal health policies have catalyzed the use of data to transform healthcare. The HITECH Act was implemented as part of the American Recovery and Reinvestment Act of 2009 to invest $28 billion in the adoption and use of health information technology. Most hospitals and physicians in the United States now have electronic systems to aggregate patient data for billing and clinical processes. Most large hospitals (500+ beds) have purchased one of two electronic health record (EHR) platforms, Cerner or Epic. Considering the large share of patients with insurance coverage from the federal government, the Patient Protection and Affordable Care Act of 2010 established The Centers for Medicare & Medicaid Services (CMS) Innovation Center, which prioritizes the timely and actionable use of this digital health data to improve quality of care and control costs.
The increased availability of data introduced the “Big Data Revolution” in healthcare with promises of dramatic breakthroughs in population health, disease management, and personalized medicine.[32] Some healthcare systems have managed to collect, analyze, learn from, and act on data from medical encounters for decades.[33] But many are challenged to make meaningful use of the vast amounts of data that are captured and stored. Some of the hindrances include the fact that disparate sources of health data are needed to create a complete picture of patient experiences (including ambulatory care data, inpatient discharge data, insurance claims data, EHR data, and clinical notes), leading to a lack of interoperability (the ease of different information systems to access, exchange, and utilize data) which is often due to the proprietary nature of EHR vendor systems. In short, the introduction and operationalization of EHR data into a health care system is the work of generations, and the widespread adoption of the digital interface without interruption to workflow takes many years. Notably, efforts to universally transfer health systems over to a digital format have not always gone smoothly and offer important lessons that must consider both patient and provider perspectives and needs.[34][35]
The collection and orchestration of patient-reported data to drive patient-centered, high-quality care
One example of a successful integration of patient data to improve care has been demonstrated by addressing SDOH factors directly at the point of care. The current Healthy People 2030 Initiative,[36] which began in 1979 as a health.gov data-driven nationwide objective to improve population health, has most recently distilled the social determinants of health into five distinct domains; educational access and quality, healthcare access and quality, neighborhood and built environment, social and community contacts, and economic stability.
To effectively manage these upstream SDOH factors, the American College of Physicians published a position paper in 2018 on nine specific actionable areas to improve social determinants of health in order to have a beneficial and sustainable impact on patient care.[37] Four action areas fall in the realm of policy, allocation of funding, and payment models, and the remaining action areas focus on screening in clinical practice, research and educational efforts, interprofessional communication and collaboration, and the development of best practices to improve utilization of EHR systems. A recent study in a federally qualified health center demonstrated that barriers to implementation of social needs screening in primary care medical clinics included resource availability, administrative burden, and discrimination. The same study identified facilitating factors to include team-based staffing models, evidence-based clinical techniques for shared decision-making, and clinicians’ perceptions that SDOH screening aligns with patient-centered care.[38] Patient needs that are most commonly and consistently reported across national cohorts or smaller studies of community clinics include depression/medium-high stress, lack of insurance, low education, unemployment, and lack of physical activity.[39][40][41] A large multi-site, cross-sectional study across nine states observed that lower income was the patient characteristic that was most strongly associated with an interest in receiving support for social need.[42]
While certain technological advances such as telemedicine may provide ease and availability to essential services that can expand reach, it is also critical to ensure that a digital divide doesn’t further reinforce health disparities.
The transition to a hospital-wide electronic health system in the author’s institution occurred a decade ago. Almost five years ago, CMS initiated Medicaid Managed Services to introduce regular screening for SDOH factors in an effort to mitigate social risk factors during primary care encounters for individuals receiving Medicaid services.[43] SDOH screening was implemented across the hospital network and more importantly, processes were developed to offer immediate services addressing suicide risk protocols, depression and substance misuse, and unmet basic needs. Trained personnel were hired to provide this “bridge role,” including social workers, behavioral health counselors, and community health workers.
While common subclinical stressors may be effectively addressed by SDOH screening, the Collaborative Care Model is an evidence-based strategy to manage more complex psychosomatic conditions in the primary care setting.[44]This data-driven approach to integrated mental health care has demonstrated widespread efficacy across various healthcare systems and payment models and has proven effective to the challenges of COVID-19 pandemic restrictions to traditional in-person health services through the adaptation to telemedicine.[45] The Collaborative Care Model has also been implemented at our institution and has provided routine mental health screening to address moderate to severe depression and anxiety symptoms in the primary care setting. The integration of patient-reported mental health symptoms from various sources (patient home portals, entry surveys, behavioral health clinician reports, or clinical notes) allows patients immediate access to trained behavioral health clinicians to receive psychologic counseling. Efforts are currently underway to determine not only the clinical effectiveness but also cost effectiveness of these innovative models of integrated care to address mental health as a central component of optimal patient wellbeing.
Novel EHR-based tools to combat clinician burnout
Considerable attention must also be paid to the enormous impact the COVID-19 pandemic continues to have on the health and wellbeing of healthcare workers in this country and globally. Not surprisingly, a recent international review of healthcare workers demonstrated high rates of PTSD, anxiety, depression, and distress due to the pandemic.[46] While many factors may contribute, lack of control at work and risk of working with patients with COVID-19 were among the risk factors associated with the development of mental health disorders among clinical staff.[47] In a recent study on the risk of infection from SARS-CoV-2 among clinicians, a 2.7 fold increased risk was demonstrated if providers cared for 10-50 COVID-19 patients compared to providers who cared for less than ten COVID-19 patients over the nine-month study period.[48] This risk was more than four times higher if providers had cared for more than 50 patients diagnosed with COVID-19. No statistical difference in risk was observed between physicians and advanced practice providers.[49]
Considering the high cost of burnout among hospital workers during the current pandemic, it is more important now than perhaps ever before to implement approaches to improve the working conditions of our essential healthcare providers. At our institution, efforts were initiated in 2016 to implement an EHR-based tool for the consistent and fair assignment of nursing staff.[50] Intolerable workload has long been a key driver of nursing attrition and was therefore the target of the development of a nursing workload scoring system that could automate staffing allocation based on patient need already captured four times daily in the medical records. This routinely updated patient workload score reflects the work experience—in real time—associated with each individual patient. By incorporating the individual patient workload score into a calculation that accounts for department staffing ratios, equitable assignment of available staff can be matched to patient demand. Rollout of this staffing tool to other hospitals within our network has been interrupted by staffing shortages and increased need for care due to the COVID-19 pandemic.
Public health messaging needs to involve community members and trusted organizations as essential contributors and direct lines of communication to populations.
In summary, the integration of EHR data into clinical care has been shown to improve processes of care for both patients and providers. Particularly, the incorporation of patient-reported measures of both mental health and social risk into clinical management is essential to make real advances in health equity.[51] Optimizing the use of health data to improve care is a challenge. Researchers and medical institutions are hindered by the scarcity of available resources (both financial and computing) as well as limited professional and technological expertise to integrate and manage the tremendous volume of data derived from disparate sources. The protection of patient privacy is of foremost importance, and along with the ownership and governance of health data, contributes to privacy and security concerns which also limit the ability to fully realize the potential of health data. The widespread adoption of digital health data infrastructures across healthcare systems in the United States offered little protection against the spread of SARS-CoV-2 and the devastating impact that the pandemic has had on many members of our communities. The noticeable shortcomings reveal opportunities for new training that are needed on many levels; to educate clinicians on the importance of social risk as much as biomedical risks,[52] to increase the capacity of computer programmers and statisticians to meaningfully analyze data as well as data architects to collect and manage it, and to integrate non-medically trained practitioners into health management teams to share in the collective responsibility of serving all needs of our patients and populations.
Moving forward
Perhaps the most essential truth that the current pandemic has exposed is that our individual health depends on our collective health. While certain technological advances such as telemedicine may provide ease and availability to essential services that can expand reach, it is also critical to ensure that a digital divide doesn’t further reinforce health disparities.[53] Moving forward as spread of SARS-CoV-2 becomes more endemic with anticipated seasonal and holiday-related waves, it will be critical to support the more biologically accurate public health message of masking and physical distancing—to limit viral transmission but maintain social connection—so as not to severely impact individual mental wellbeing. Moreover, individual risk must be weighed against community risk and considered in the context of regional viral prevalence. The use of terms such as “fully vaccinated” and “waning immunity” are potentially misleading given ever-evolving host-pathogen interactions and the incomplete picture antibody measurements offer for the full capacity of the human immune response.[54] Thus public health messaging should be informed by the scientific community with evidence- based knowledge from members of diverse fields of science including immunologists and virologists.
The exchange of effective communication strategies will be critical as SARS-CoV-2 becomes more endemic. An interdisciplinary approach that includes medical anthropologists and social scientists is also critically important to improve effective public health communication approaches. Additionally, the integration of database platforms will be needed to evaluate both upstream policies and population behaviors with downstream indicators of individual physical, economic, and social wellbeing.[55] Public health messaging needs to involve community members and trusted organizations as essential contributors and direct lines of communication to populations. We have witnessed first metropolitan, then rural, and now trans-regional spread of this novel coronavirus.[56] Looking forward, we have much to learn from successes and failures of public health messaging and perhaps most importantly we have to consider how best to tailor messages to the regional needs of affected populations. By using geospatial analyses, public health efforts can target specific neighborhoods and regions through established community outreach programs. The regional variation in vaccination rates remains high across the United States as in other countries. To increase vaccine uptake and/or public health measures to limit viral spread, a balance of individual and community priorities should be encouraged through a perspective centered in social justice and antiracism. And finally, to ensure global health, resource allocation must be equitably managed. With concerns of emerging variants and global vaccine distribution, examples of national generosity and internationally coordinated efforts to distribute healthcare resources and medical technologies are imperative to create communities where all individuals can flourish and have a chance to achieve their full potential.[57][58][59]
Literature
[1] Warnick A. Interest in public health degrees jumps in wake of pandemic: Applications rise. The Nation’s Health. 2021;51(6):1-12.
[2] Jones CP, Jones CY, Perry GS, Barclay G, Jones CA. Addressing the social determinants of children’s health: a cliff analogy. J Health Care Poor Underserved. 2009;20(4 Suppl):1-12.
[3] Jones CP. Overcoming Helplessness, Overcoming Fear, Overcoming Inaction in the Face of Need. American journal of public health. 2016;106(10):1717-1717.
[4] CDC. The Public Health System and the 10 Essential Public Health Services. http://www.cdc.gov/nphpsp/essentialservices.html. Accessed 11/29/21.
[5] Hekler E, Tiro JA, Hunter CM, Nebeker C. Precision Health: The Role of the Social and Behavioral Sciences in Advancing the Vision. Annals of behavioral medicine : a publication of the Society of Behavioral Medicine. 2020;54(11):805-826.
[6] Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real time. The Lancet Infectious Diseases. 2020;20(5):533-534.
[7] Branswell H. CDC details first U.S. case of novel virus spreading in China. STAT. Jan. 21, 2020. https://www.statnews.com/2020/01/21/cdc-expected-to-detail-first-u-s-case-of-novel-virus-spreading-in-china/
[8] Lee J, Pullin, R. South Korea confirms first case of new coronavirus in Chinese visitor. Reuters. Jan. 19, 2020. https://www.reuters.com/article/us-china-health-pneumonia-south-korea-idUSKBN1ZJ0C4
[9] Islam N, Jdanov DA, Shkolnikov VM, et al. Effects of covid-19 pandemic on life expectancy and premature mortality in 2020: time series analysis in 37 countries. BMJ. 2021;375:e066768.
[10] Parikh S, O’Laughlin K, Ehrlich HY, et al. Point Prevalence Testing of Residents for SARS-CoV-2 in a Subset of Connecticut Nursing Homes. JAMA : the journal of the American Medical Association. 2020;324(11):1101-1103.
[11] Lee S, Kim T, Lee E, et al. Clinical Course and Molecular Viral Shedding Among Asymptomatic and Symptomatic Patients With SARS-CoV-2 Infection in a Community Treatment Center in the Republic of Korea. JAMA internal medicine. 2020;180(11):1447-1452.
[12] Senatore V, Zarra T, Buonerba A, et al. Indoor versus outdoor transmission of SARS-COV-2: environmental factors in virus spread and underestimated sources of risk. Euro-Mediterranean journal for environmental integration. 2021;6(1):30.
[13] Adhikari SP, Meng S, Wu Y-J, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(1):29-29.
[14] Jain V, Yuan JM. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: a systematic review and meta-analysis. Int J Public Health. 2020;65(5):533-546.
[15] Boden M, Cohen N, Froelich JM, Hoggatt KJ, Abdel Magid HS, Mushiana SS. Mental disorder prevalence among populations impacted by coronavirus pandemics: A multilevel meta-analytic study of COVID-19, MERS & SARS. General hospital psychiatry. 2021;70:124-133.
[16] Emeny RT, Carpenter DO, Lawrence DA. Health disparities: Intracellular consequences of social determinants of health. Toxicol Appl Pharmacol. 2021:115444.
[17] Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis. 1992;2(3):207-221.
[18] Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310-357.
[19] Marmot M. Socioeconomic determinants of CHD mortality. Int J Epidemiol. 1989;18(3 Suppl 1):S196-202.
[20] Davenhall WF, Kinabrew C. GIS in Health and Human Services. Springer Handbook of Geographic Information. 2012:557-578.
[21] Wennberg J, Gittelsohn. Small area variations in health care delivery. Science. 1973;182(4117):1102-1108.
[22] WHO. Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. 2008; https://www.who.int/social_determinants/final_report/csdh_finalreport_2008.pdf. Accessed 11/29/21.
[23] Friedman S, Lee J-W. COVID-19 Mortality in New York City Across Neighborhoods by Race, Ethnicity, and Nativity Status. Geographical Review. 2021;111(4):571-591.
[24] Hekler E, Tiro JA, Hunter CM, Nebeker C., 2020
[25] WHO. World Health Organization Remains Firmly Committed to the Principles Set Out in the Preamble to the Constitution. https://www.who.int/about/governance/constitution. Accessed 12/07/21.
[26] Hekler E, Tiro JA, Hunter CM, Nebeker C., 2020
[27] Artiga S., Hinton E., Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity. The Kaiser Commission on Medicaid and the Uninsured; 2015. https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101740257-pdf
[28] Keisler-Starkey K, Bunch, L.N. Health Insurance Coverage in the United States: 2020. Current Population Reports, P60-274. 2021.
[29] Ramgobin D, McClafferty B, Kramer C, Golamari R, McGillen B, Jain R. Papering over the cracks: COVID-19’s amplification of the failures of employer-based health insurance coverage. J Community Hosp Intern Med Perspect. 2021;11(1):107-110.
[30] Owens PL. COVID-19-Related Hospitalizations in 13 States, by Expected Payer, 2020: Statistical Brief #274. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2021.
[31] Keisler-Starkey K, Bunch, L.N., 2021.
[32] Harris Y, Schneider C. Big Data: A Realistic Assessment of Its Applications to Health Care. Health Information Technology in the United States 2015. Robert Wood Johnson Foundation. Princeton, N.J.2015.
[33] Dean NC, Jones BE, Jones JP, et al. Impact of an Electronic Clinical Decision Support Tool for Emergency Department Patients With Pneumonia. Annals of emergency medicine. 2015;66(5):511-520.
[34] U.S. Dept Veterans Affairs. VA advances Electronic Health Record Modernization program. 2021; https://www.va.gov/opa/pressrel/pressrelease.cfm?id=5745. Accessed 12/01/21.
[35]Huang C, Koppel R, McGreevey JD, 3rd, Craven CK, Schreiber R. Transitions from One Electronic Health Record to Another: Challenges, Pitfalls, and Recommendations. Applied clinical informatics. 2020;11(5):742-754.
[36]Gomez CA, Kleinman DV, Pronk N, et al. Addressing Health Equity and Social Determinants of Health Through Healthy People 2030. J Public Health Manag Pract. 2021;27(Suppl 6):S249-S257.
[37]Daniel H, Bornstein SS, Kane GC. Addressing Social Determinants to Improve Patient Care and Promote Health Equity: An American College of Physicians Position Paper. Ann Intern Med. 2018;168(8):577-578.
[38]Drake C, Batchelder H, Lian T, et al. Implementation of social needs screening in primary care: a qualitative study using the health equity implementation framework. BMC health services research. 2021;21(1):975.
[39]Weir RC, Proser M, Jester M, Li V, Hood-Ronick CM, Gurewich D. Collecting Social Determinants of Health Data in the Clinical Setting: Findings from National PRAPARE Implementation. J Health Care Poor Underserved. 2020;31(2):1018-1035.
[40]Tou LC, Prakash N, Jeyakumar SJ, Ravi S. Investigating Social Determinants of Health in an Urban Direct Primary Care Clinic. Cureus. 2020;12(10):e10791.
[41]Kusnoor SV, Koonce TY, Hurley ST, et al. Collection of social determinants of health in the community clinic setting: a cross-sectional study. BMC Public Health. 2018;18(1):550.
[42]De Marchis EH, Hessler D, Fichtenberg C, et al. Assessment of Social Risk Factors and Interest in Receiving Health Care-Based Social Assistance Among Adult Patients and Adult Caregivers of Pediatric Patients. JAMA Netw Open. 2020;3(10):e2021201.
[43]Machledt D. Addressing the Social Determinants of Health Through Medicaid Managed Care. Issue Brief 2017; https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_2017_nov_machledt_social_determinants_medicaid_managed_care_ib_v2.pdf.
[44]Unützer J, Katon W, Callahan CM, et al. Collaborative Care Management of Late-Life Depression in the Primary Care SettingA Randomized Controlled Trial. JAMA : the journal of the American Medical Association. 2002;288(22):2836-2845.
[45]Carlo AD, Barnett BS, Unützer J. Harnessing Collaborative Care to Meet Mental Health Demands in the Era of COVID-19. JAMA Psychiatry. 2021;78(4):355-356.
[46]Saragih ID, Tonapa SI, Saragih IS, et al. Global prevalence of mental health problems among healthcare workers during the Covid-19 pandemic: A systematic review and meta-analysis. Int J Nurs Stud. 2021;121:104002.
[47]Riedel B, Horen SR, Reynolds A, Hamidian Jahromi A. Mental Health Disorders in Nurses During the COVID-19 Pandemic: Implications and Coping Strategies. Frontiers in public health. 2021;9:707358.
[48]Sacks OA, Barnato AE, Skinner JS, Birkmeyer JD, Fowler A, Birkmeyer N. Elevated Risk of COVID-19 Infection for Hospital-Based Health Care Providers. Journal of general internal medicine. 2021;36(11):3642-3643.
[49]Sacks OA, Barnato AE, Skinner JS, Birkmeyer JD, Fowler A, Birkmeyer N., 2021
[50]Meyer KR, Fraser PB, Emeny RT. Development of a Nursing Assignment Tool Using Workload Acuity Scores. J Nurs Adm. 2020;50(6):322-327.
[51]Gallo JJ, Joo JH, Visvanathan K, McGinty EE, Thrul J, Holingue C. An Idea Whose Time Has Come: Promoting Health Equity by Preventing the Syndemic of Depression and Medical Comorbidity. The American journal of geriatric psychiatry : official journal of the American Association for Geriatric Psychiatry. 2021;29(1):12-14.
[52]FitzPatrick ME, Badu-Boateng C, Huntley C, Morgan C. ‘Attorneys of the poor’: Training physicians to tackle health inequalities. Future Healthcare Journal. 2021;8(1):12-18.
[53]Garber J. Digital redlining: How telehealth can exacerbate inequalities. Health Equity 2021; https://lowninstitute.org/digital-redlining-how-telehealth-can-exacerbate-inequalities/. Accessed 10/15/21.
[54]Bender M. Changing the definition of ‘fully vaccinated’ is more than just semantics, experts argue. STAT 2021; https://www.statnews.com/2021/12/08/changing-definition-fully-vaccinated-more-than-semantics/?utm_source=STAT+Newsletters&utm_campaign=a302499e85-MR_COPY_01&utm_medium=email&utm_term=0_8cab1d7961-a302499e85-152057049. Accessed 12/08/21.
[55]Oliver BJ, Schmidt P, Tomlin S, Kraft SA, Fisher E, Nelson EC. A ‘COVID Compass’ for navigating the pandemic. International Journal for Quality in Health Care. 2021;33(Supplement_2):ii78-ii80.
[56]Schmidt P, Nelson EC, Kearney G, Kraft S, Oliver BJ. International, national and local trends in the spread of COVID-19: a geographic view of COVID-19 spread and the role to be played by coproduction. International Journal for Quality in Health Care. 2021;33(Supplement_2):ii71-ii77.
[57] Jones CP, Jones CY, Perry GS, Barclay G, Jones CA., 2009.
[58] Jones CP., 2016.
[59]Nebehay S. Swiss strike deal for COVAX to get 1 mln Moderna doses more quickly. Reuters 2021; https://www.reuters.com/business/healthcare-pharmaceuticals/swiss-strike-deal-covax-get-1-mln-moderna-doses-more-quickly-2021-11-24/?utm_source=Nature+Briefing&utm_campaign=9334111e0a-briefing-dy-20211125&utm_medium=email&utm_term=0_c9dfd39373-9334111e0a-45210706. Accessed 12/07/21.
This article is part of the AGI project “The Importance of the Transatlantic Partnership in Times of Global Crises” and is generously funded by the Transatlantik-Programm der Bundesrepublik Deutschland aus Mitteln des European Recovery Program (ERP) des Bundesministerium für Wirtschaft und Energie (BMWi) (Transatlantic Program of the Federal Republic of Germany with Funds through the European Recovery Program (ERP) of the Federal Ministry for Economics and Energy (BMWi)).




